1. Name of the location of 90% of epistaxis
2. A genetic disorder that forms AV malformations in the skin, lungs, brain etc
3. Name of posterior vascular plexus in the nasal cavity causing posterior epistaxis
4. 1st line treatment for all epistaxis
5. The common brand name for anterior nasal packing
6. Chemical used in cautery sticks
7. Physically scaring complication of posterior nasal packing with foleys catheter
Coming soon..

The Facial Nerve
In this tutorial, you will learn about the anatomy of the facial nerve. This nerve supplies the muscles of the face that are concerned with facial expressions. Smiling, frowning, blinking the eye and whistling are just some of the movements that the facial nerve allows us to do.
The importance of the facial nerve to us as clinicians is that diseases of the ear may damage it and cause paralysis. The clinician must, therefore, recognize the presence of paralysis as it implies serious ear disease such as cholesteatoma. The state of facial nerve function should always be noted when we examine an ear.
ANATOMICAL OVERVIEW
The facial nerve is one of the cranial nerves. Cranial nerves are nerves that come directly out of the brain. These are different to the nerves that move our arms or legs as those nerves come out of the spinal cord.
There are twelve cranial nerves and they do jobs like moving the eyes, moving the face, moving the tongue and shoulders, feeling pain in the face, detecting light, balance and sound and many other jobs. There is a list of the cranial nerves in the table below. You don’t have to worry about them all at this time although they will become important in the future. For now just take a look at the sorts of things that cranial nerves do.

The next few pictures show the cranial nerves as they appear under the brain and in real life.
This is a view of the underside of the brain (inferior side). It shows the cranial nerves.
Notice that the nerves are paired – that is that there is one on each side of the brain.
All of the nerves come directly out of the brain but the only one does not leave the skull. It is the olfactory nerve.
All of the others leave the skull through holes in the bone of the skull called foramina.

This is the inferior surface of an actual human brain. It shows the cranial nerves emerging from the brain. They are white in colour
The course of the facial nerve (the pathway that it follows from the brain into the facial muscles) is very complicated. However, what is important for us is that it passes with the vestibulocochlear nerve into the inner ear (cranial nerve 8), it then passes through the middle ear and mastoid before leaving the skull. Once out of the skull it travels inside the parotid salivary gland to get to the muscles in the face.
In other words, the facial nerve travels through areas of the body that ear clinicians examine and test every day. Diseases such as cholesteatoma, acute otitis media and acoustic neuroma can affect the facial nerve so we must know about the nerve and be able to examine it.
The anatomy of the Facial nerve (Cranial nerve 7)
When we describe the course of the facial nerve we divide it into segments[1]. We will look at three of these: the intracranial segment, the intratemporal segment and the extratemporal segment.
The intracranial segment
This segment is that part of the nerve that lies inside the skull itself before it passes into the middle ear. Once the nerve has left the brain it passes into the internal acoustic meatus (IAM). In the IAM it runs with the cochlear nerve and the vestibular nerves.


This is a picture looking up through the internal acoustic meatus on the right side.
Imagine that you are standing inside the head looking out into it.
Superiorly there are two holes. The anterior one takes the facial nerve and the posterior one takes the superior vestibular nerve.
Inferiorly and anteriorly is the spiral foramina that takes the cochlear nerve while posteriorly is the foramen for the inferior vestibular nerve.
This diagram is a simpler way of looking at the anatomy.
S, I, A, and P are superior, inferior, anterior and posterior.
VII is Cranial nerve 7 – the facial nerve.
SV and IV are the superior and inferior vestibular nerves
C is the cochlear nerve
Figure: Two pictures that show the IAM and how the nerves pass through it.
Acoustic neuromas and fractures of the temporal bone can damage the nerve in this segment.
Once the nerve passes into its foramen it leaves the intracranial segment and enters the intratemporal segment.
The intratemporal segment
This is the segment of the nerve that lies inside the middle ear and mastoid. This is a very important part of the nerve because it is the part that is affected by middle ear diseases such as otitis media and cholesteatoma. These are diseases that you see all of the time.
In the middle ear the facial nerve starts anteriorly and then runs posteriorly and then inferiorly. It is a complicated course that passes by the promontory, the tensor tympani, the stapes, and the pyramid of the stapedius muscle. You only need to know all of this when you are actually operating on the ear so don’t worry too much about all of these new names.

You saw this picture in the tutorial on the middle ear. It shows the middle ear seen without a tympanic membrane and with the scutum removed.
The picture below shows a facial nerve in the middle ear in a yellow colour. The facial nerve enters the middle ear just superior to the cochlea at A. It then passes posteriorly in the middle ear to lie just superior to the oval window (B). At this point it turns inferiorly so that it comes to lie posterior to the oval window and the round window (C).
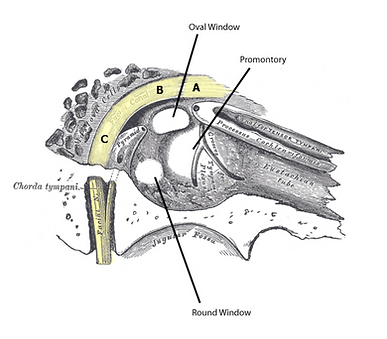
While in the middle ear the facial nerve gives off two special nerves. One is the nerve to stapedius and the other is the chorda tympani. The nerve to stapedius is responsible for making stapedius muscle contract when the ear is exposed to very loud sound (acoustic reflex). The chorda tympani carries taste information from the tongue to the brain.
From posterior to the oval window the nerve travels inferiorly and out of the temporal bone at the stylomastoid foramen. It is then in its extratemporal segment.
The extratemporal segment
This is where the nerve divides into five branches. Each of these is responsible for moving a part of the face. In the image below you can see these branches on the side of the face. The ones that move the muscles in the face are shown in yellow.

You can see that they supply muscles around the eye so that you can raise your eyebrows or close your eyes.
They go to the muscles around the lips and allow you to smile and keep your lips closed.
They also go into the neck muscles.
Facial Palsy
If a disease within the middle ear (such as cholesteatoma) damages the nerve the face will become weak because the muscles will not move. Below is a picture of a patient trying to smile.

Notice how the right side of his face moves normally but that the left side does not move at all. He has a weakness of the left facial nerve of the type that could be caused by middle ear disease.
The medical term for this weakness is palsy.
Patients with complete facial nerve palsy cannot blink and this means that their eyes can become damaged and may even become blind. Looking after the eye is important and it must be kept closed with an eye patch until the nerve starts to recover its function. Eye drops are also useful to prevent drying of the eye’s surface.
There are many diseases that can cause facial nerve palsy apart from middle ear diseases. A list of the diseases that you may encounter is shown in the table but there are many other rarer causes.

Patients with complete facial nerve palsy cannot blink and this means that their eyes can become damaged and may even become blind. Looking after the eye is important and it must be kept closed with an eye patch until the nerve starts to recover its function. Eye drops are also useful to prevent drying of the eye’s surface.
There are many diseases that can cause facial nerve palsy apart from middle ear diseases. A list of the diseases that you may encounter is shown in the table but there are many other rarer causes.

Examining the facial nerve
Examining the face is easy. Ask the patient to raise their eyebrows, close their eyes tightly, to smile and to whistle or puff their cheeks out. Look at both sides of the face when they are doing this and compare them. Make a record of what you see.
Learning points:
-
Whenever you see a patient with ear disease you should examine the facial nerve. This is particularly true of patients with perforations and cholesteatomas
-
The opposite is also true; whenever you see a patient with a facial palsy you must examine the ear because the cause of the palsy may be an ear disease
-
Always keep a written record of what you see
-
If you see a patient with middle ear disease and a facial palsy they need to see an ear surgeon as an emergency
-
Always protect the eye while a facial palsy is present because blindness is a possibility due to scarring of the eye’s surface
-
A stroke can look very similar but the forehead will not be weak

Disclaimer
This site is for educational purposes only and as such does not replace clinical judgement. The site contains high-resolution images, although mobile compatible. For optimum viewing, please switch to a HD ready computer.
