1. Name of the location of 90% of epistaxis
2. A genetic disorder that forms AV malformations in the skin, lungs, brain etc
3. Name of posterior vascular plexus in the nasal cavity causing posterior epistaxis
4. 1st line treatment for all epistaxis
5. The common brand name for anterior nasal packing
6. Chemical used in cautery sticks
7. Physically scaring complication of posterior nasal packing with foleys catheter
Coming soon..

Anatomical Terms
In this tutorial, you will learn the common terms that we use when describing eardrum anatomy and pathology. First some simple anatomical terms will be discussed and following this some terms that we only use for ear disease. At the end is a short quiz to test yourself.
ANATOMICAL TERMS
Anatomy has its own special language and you must know some of it before you start. The terms that you most frequently hear are: medial, lateral, superior, inferior, anterior, posterior and midline.

Midline - This is an imaginary line that runs right through the middle of our bodies from head to toe.
Medial - When a structure lies medial (or medially) to another structure it lies closer to the midline of the body. For example the cochlea lies medial to the eardrum because it is nearer the midline of the body. Another example is the stapes lies medial to the malleus.
Lateral - this is the opposite of medial so the structure lies further from the midline. The pinna lies lateral to the eardrum and the incus lies lateral to the stapes.
Superior - if one structure is superior to another it lies nearer the top of the head. For example the eyes are superior to the mouth and the temporal lobe of the brain lies superior to the middle ear.
Inferior - this is the opposite of superior. If one structure is inferior to the other it lies closer to the feet. For example the stomach is inferior to the oesophagus and the tongue is inferior to the nose.
Anterior - this means that the structure lies nearer the front of the body. For example the Eustachian tube lies anterior to the cochlea and the teeth lie anterior to the tonsils.
Posterior - this is the opposite of anterior. The oval window lies posterior to the promontory and the mastoid lies posterior to the middle ear.
With these words you can describe the relationship of any structure in the human body to any other structure. You can also describe the position of perforations on the eardrum, where retractions or scars are and where other diseases are found.
THE EARDRUM
When we describe abnormalities on the eardrum we use similar words but in a slightly different way. In the diagram below I have drawn a line down the handle of the malleus. The line slopes as it passes downwards. In otology we use this line to decide what is anterior and what is posterior on the drum. Similarly we draw a line across the first line to define what is superior and what is inferior.

This may be a little different from what you have seen before but don’t worry about it. With these lines in place we can now describe the position of all abnormalities on the eardrum. In the following diagram I have coloured the eardrum to illustrate the relations

This all leads to you being able to describe the drum accurately. In the drum below I have coloured all the quadrants (quarters of the drum) differently.

Sometimes a disease will spread into two or more quadrants. If it does you can say that it is in the posterior half of the drum (if it is in both the superior and inferior posterior quadrants) or the inferior half if it is in both the anterior and posterior inferior quadrants. The following clinical pictures show how you can describe the position of a perforation or other abnormality.
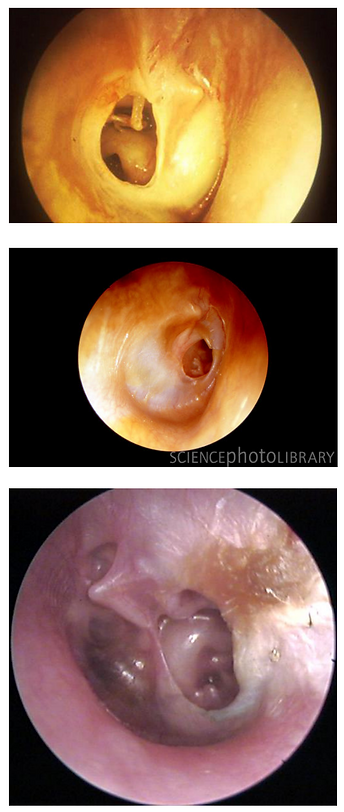
Posterior perforation.
This perforation is too big to be in one quadrant so we say that it is large and posterior. It is also central because there is some drum all around it (see below).
The incus, stapedius and round window niche are all seen through the perforation.
Antero-superior central perforation.
This perforation is limited to one quadrant.
Posterior retraction.
This looks like a perforation but it is a retraction. It is too big to be in one quadrant so it is called a large posterior retraction.
There is crust coming out of it and this tells us that there is an underlying infection – probably a cholesteatoma hidden from view.
TYPES OF PERFORATION
Knowing how to describe where a perforation is situated is just the first step. Next you must decide whether it is central or marginal.
Central perforations – these are holes in the eardrum that have some tissues all around them. Please note that the word ‘central’ does not mean that the hole is in the middle of the eardrum.
Marginal perforations – these do not have tissues all around them. On one side there will be bone.
Attic perforations – these are found superiorly in the pars flaccida. They are almost always marginal.
Look at the following diagrams. They show eardrums and the blue marks represent perforations (real perforations aren’t blue of course).

Here we can see two perforations. Both are central.
The anterior one is small and situated in the antero-inferior quadrant. It has eardrum tissues all around it
The posterior one is large but it is still central – there is some eardrum all around it.
Neither of these is in the middle of the eardrum.
Here there are two more perforations. The superior one is an attic perforation and it is marginal because there is no drum superior to it.
The posterior one is a posterior marginal perforation. There is only drum on one side of it and there is bone on the other side. This is how a marginal perforation is defined.
This is just an introduction to anatomical terms. Others will emerge through your learning as you progress through the tutorials presented here.

Disclaimer
This site is for educational purposes only and as such does not replace clinical judgement. The site contains high-resolution images, although mobile compatible. For optimum viewing, please switch to a HD ready computer.
